What Harm Causes the Epidural to the Baby
The extract from this article was originally published by Dr. Sarah J. Buckley in 2005 at world wide web.sarahbuckley.com | Previously published in Mothering No.133, Nov-Dec 2005, as "The Hidden Risks of Epidurals" Eastpidurals involve the injection of a local anesthetic drug (derived from cocaine) into the epidural space—the space effectually (epi) the tough coverings (dura) that protect the spinal string. A conventional epidural will numb (cake) both the sensory and motor nerves every bit they exit from the spinal cord, giving very effective pain relief for labor merely making the recipient unable to motion the lower part of her body. In the last five to 10 years, epidurals have been adult with lower concentrations of local anesthetic drugs, and with combinations of local anesthetics and opiate hurting killers (drugs like to morphine and meperidine) to reduce the motor block, and to produce a so-called "walking" epidural. Southwardpinal analgesia has also been increasingly used in labor to reduce the motor block. Spinals involve drugs injected right through the dura and into the spinal (intrathecal) space, and produce only curt-term analgesia. To prolong the pain-relieving effect for labor, epidurals are now being co-administered with spinals, equally a combined spinal epidural (CSE). Epidurals and spinals offer laboring women the most effective form of hurting relief available, and women who have used these analgesics rate their satisfaction with pain relief as very high. However, satisfaction with pain relief does not equate with overall satisfaction with nativity, and epidurals are associated with major disruptions to the processes of nascency. These disruptions can interfere with a woman's ultimate enjoyment of and satisfaction with her labor experience, and may also compromise the rubber of birth for mother and babe. Epidurals significantly interfere with some of the major hormones of labor and birth, which may explain their negative effect on the processes of labor.6 As the World Health System comments, "epidural analgesia is 1 of the most hit examples of the medicalization of normal birth, transforming a physiological event into a medical procedure." For example, oxytocin, known equally the hormone of love, is besides a natural uterotonic—a substance that causes a woman's uterus to contract in labor. Epidurals lower the mother's production of oxytocin, or finish its normal rise during labor. The outcome of spinals on oxytocin release is fifty-fifty more marked. Epidurals also obliterate the maternal oxytocin peak that occurs at birth —the highest of a female parent's lifetime—which catalyses the terminal powerful contractions of labor and helps mother and baby to fall in love at kickoff meeting. Some other important uterotonic hormone, prostaglandin F2 alpha, is also reduced in women using an epidural. Beta-endorphins are the stress hormones that build upward in a natural labor to help the laboring adult female to transcend pain. Beta-endorphins are as well associated with the altered state of consciousness that is normal in labor. Being "on another planet," equally some describe it, helps the female parent-to-be to work instinctively with her torso and her infant, often using movement and sounds. Epidurals reduce the laboring woman's release of beta-endorphins. Perhaps the widespread use of epidurals reflects our difficulty with supporting women in this altered land, and our cultural preference for laboring adult female to be placidity and acquiescent. Adrenaline and noradrenaline (epinephrine and norepinephrine, collectively known every bit catecholamines, or CAs) are also released under stressful conditions, and levels naturally increase during an unmedicated labor. At the end of an undisturbed labor, a natural surge in these hormones gives the mother the free energy to push her baby out, and makes her excited and fully alert at get-go meeting with her babe. This is known as the fetal ejection reflex. However, labor is inhibited by very high CA levels, which may exist released when the laboring woman feels hungry, cold, fearful, or unsafe.17 This makes evolutionary sense: If the mother senses danger, her hormones will slow or stop labor and give her the time to flee to find a safer place to birth. Epidurals reduce the laboring woman's release of CAs, which may exist helpful if high levels are inhibiting her labor. Withal, a reduction in the final CA surge may contribute to the difficulty that women laboring with an epidural can experience in pushing out their babies, and the increased chance of instrumental delivery (forceps and vacuum) that accompanies the use of an epidural (see below). Eastwardpidurals boring labor, possibly through the above furnishings on the laboring woman's oxytocin release, although there is likewise testify from fauna research that the local anesthetics used in epidurals may inhibit contractions by directly affecting the muscle of the uterus.18 On average, the get-go stage of labor is 26 minutes longer in women who use an epidural, and the second, pushing phase is 15 minutes longer. Loss of the final oxytocin peak probably also contributes to the doubled risk of an instrumental delivery—vacuum or forceps—for women who employ an epidural, although other mechanisms may be involved. For case, an epidural likewise paralyses the laboring adult female's pelvic floor muscles, which are important in guiding her baby's head into a good position for birth. When an epidural is in identify, the baby is four times more likely to be persistently posterior (POP or face up) in the final stages of labor—in 1 report, 13 per centum compared to 3 percent for women without an epidural. A POP position decreases the chance of a spontaneous vaginal delivery (SVD). In one study, only 26 percent of first-fourth dimension mothers (and 57 percent of experienced mothers) with POP babies experienced a SVD; the remaining mothers had an instrumental birth (forceps or vacuum) or a cesarean. Anesthetists have hoped that a depression-dose or combined spinal epidural would reduce the chances of an instrumental delivery, merely the improvement seems to be pocket-size. In i study, the Conventional Obstetric Mobile Epidural Trial (COMET), 37 percent of women with a conventional epidural experienced instrumental births, compared with 29 percent of women using low-dose epidurals and 28 percent of women using CSEs. For the baby, instrumental commitment can increment the short-term risks of bruising, facial injury, displacement of the skull basic, and cephalohematoma (blood clot nether the scalp). The risk of intracranial hemorrhage (bleeding within the encephalon) was increased in i study by more than than four times for babies born by forceps compared to spontaneous birth, although 2 studies showed no detectable developmental differences for forceps-born children at five years quondam. Some other written report showed that when women with an epidural had a forceps delivery, the force used by the clinician to deliver the infant was nigh twice the force used when an epidural was non in place. Epidurals also increment the need for synthetic oxytocin (Syntocinin, Pitocin) to augment labor, due to the negative effect on the laboring woman'south own release of oxytocin. Women laboring with an epidural in place are well-nigh three times more probable to exist administered Pitocin. The combination of epidurals and Pitocin, both of which can crusade abnormalities in the fetal heart charge per unit (FHR) that indicate fetal distress, markedly increases the take a chance of operative commitment (forceps, vacuum, or cesarean delivery). In ane Australian survey, about one-half of commencement-fourth dimension mothers who were administered both an epidural and Pitocin had an operative delivery. The bear upon of epidurals on the risk of cesarean is controversial; differing contempo reviews suggest no increased risk and an increase in risk of 50 percent. The risk is probably most significant for women having an epidural with their first baby. Due northote that the studies used to make it at these conclusions are mostly randomized controlled trials in which the women who agree to participate are randomly assigned to either epidural or not-epidural pain relief. Non-epidural pain relief usually involves the adminstration of opiates such as meperidine (pethidine). Many of these studies are flawed from high rates of crossover—women who were assigned to nonepidurals but who ultimately did take epidurals, and vice versa. Besides, note that there are no true controls—that is, women who are not using whatsoever grade of pain relief—these studies cannot tell us about the bear on of epidurals compared to birth without analgesic drugs. The drugs used in labor epidurals are powerful plenty to numb, and usually paralyze, the mother'due south lower trunk, so it is not surprising that at that place can be meaning side effects for female parent and baby. These range from minor to life-threatening and depend, to some extent, on the specific drugs used. Thousandany of the epidural side effects mentioned beneath are not improved with low-dose or walking epidurals, because women using these techniques may still receive a substantial total dose of local coldhearted, peculiarly when continuous infusions and/or patient-controlled boluses (single large doses) are used. The add-on of opiate drugs in epidurals or CSEs can create further risks for the mother, such as pruritus (itching) and respiratory depression (see beneath). The almost mutual side upshot of epidurals is a drop in claret pressure. This effect is almost universal, and usually preempted by administering 4 fluids before placing an epidural. Fifty-fifty with this "preloading," episodes of significant low claret pressure (hypotension) occur for upward to half of all adult female laboring with an epidural,especially in the minutes post-obit the administration of a drug bolus. Hypotension tin cause complications ranging from feeling faint to cardiac arrest,37 and can also touch on the baby's claret supply (see below). Hypotension can be treated with more IV fluids and, if severe, with injections of epinephrine (adrenaline). Other mutual side effects of epidurals include: inability to pass urine (and requirement for a urinary catheter) for up to 2-thirds of women; itching of the skin (pruritus) for up to two-thirds of women administered an opiate drug via epidural; shivering for up to one in three women; sedation for around 1 in v women; and nausea and airsickness for i in xx women. Epidurals can as well cause a rising in temperature in laboring women. Fever over 100.4º F (38º C) during labor is 5 times more than likely overall for women using an epidural; this rise in temperature is more mutual in women having their first babies, and more than marked with prolonged exposure to epidurals. For example, in one written report, 7 percentage of first-time mothers laboring with an epidural were feverish after vi hours, increasing to 36 percent subsequently 18 hours. Maternal fever can have a significant effect on the baby (come across below). Opiate drugs, particularly administered as spinals, can sometimes crusade unexpected breathing difficulties for the female parent, which may come up on hours later nativity and may progress to take serious furnishings. One author comments, "Respiratory depression remains one of the most feared and least anticipated complications of . . . intrathecal [spinal] opioids." Kwhatsoever observational studies have found an association between epidural utilize and bleeding after birth (postpartum hemorrhage). For example, a big UK study institute that women were twice every bit likely to experience postpartum hemorrhaging when they used an epidural in labor. This may exist related to the increment in instrumental births and perineal trauma (causing bleeding), or may reflect some of the hormonal disruptions mentioned above, including increased risks of exposure to synthetic oxytocin. An epidural gives inadequate pain relief for x to 15 percent of women, and the epidural catheter needs to exist reinserted in about 5 per centum. For around 1 percent of women, the epidural needle punctures the dura (dural tap); this usually causes a severe headache that can last upward to 6 weeks, only tin can usually exist treated by an injection into the epidural space. More serious side furnishings are rare. If the epidural drugs are inadvertently injected into the bloodstream, local anesthetics can cause toxic effects such as slurred speech communication, drowsiness, and, at high doses, convulsions. This occurs in around 1 in 2,800 epidural insertions. Overall, life-threatening reactions occur for around one in iv,000 women. Decease associated with an obstetric epidural is very rare, merely tin can be caused by cardiac or respiratory arrest, or by an epidural abscess that develops days or weeks afterward. Later complications include weakness and numbness in 4 to 18 per 10,000 women, most of which resolve spontaneously within iii months. Longer-term or permanent problems can arise from: impairment to a nerve during epidural placement; from abscess or hematoma (blood jell), which tin can compress the spinal cord; and from toxic reactions in the covering of the spinal cord, which tin can lead to paraplegia. Due southome of the most significant and well-documented side effects for the unborn infant (fetus) and newborn derive from effects on the female parent. These include, as mentioned above, effects on her hormonal orchestration, blood pressure, and temperature regulation. Likewise, epidural drugs can cause direct toxic furnishings to the fetus and newborn, whose drug levels may be even college than the mother's drug levels. For the consummate commodity, sources and research conducted by Dr. Sarah J. Buckley, click hither. 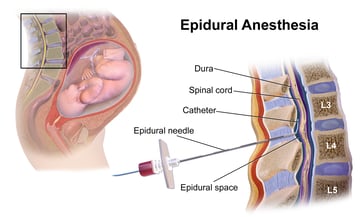 The first recorded use of an epidural was in 1885, when New York neurologist J. Leonard Corning injected cocaine into the back of a patient suffering from "spinal weakness and seminal incontinence." More than a century subsequently, epidurals have become the most popular method of analgesia, or hurting relief, in Us nascency rooms. In 2004, almost two-thirds of laboring women reported that they were administered an epidural, including 59 percent of women who had a vaginal nascency. In Canada, effectually half of women who birthed vaginally used an epidural, and in the UK, 21 percent of women had an epidural before delivery.
The first recorded use of an epidural was in 1885, when New York neurologist J. Leonard Corning injected cocaine into the back of a patient suffering from "spinal weakness and seminal incontinence." More than a century subsequently, epidurals have become the most popular method of analgesia, or hurting relief, in Us nascency rooms. In 2004, almost two-thirds of laboring women reported that they were administered an epidural, including 59 percent of women who had a vaginal nascency. In Canada, effectually half of women who birthed vaginally used an epidural, and in the UK, 21 percent of women had an epidural before delivery.Epidurals and labor hormones
Effects on the process of labor
Epidural techniques and side effects
Maternal side effects
Side effects for the baby

Source: https://www.phsmedicalsolutions.com/blog/epidural-risks-mother-baby
0 Response to "What Harm Causes the Epidural to the Baby"
Post a Comment